
ShockWave Medical: Why I am bullish on this company
ShockWave Medical: Why I am bullish on this company
$SWAV. A calcium disruptor.

Background:
Atherosclerosis means cholesterol plaque build-up inside the arteries of our body. It causes narrowing of the lumen and sometimes causes heart attack, stroke, leg pain, tissue death in the tip of the toes leading to gangrene.
About ⅓ rd of patients presenting with acute heart attack and blockage in heart arteries and half of patients presenting with blockages in leg arteries present with moderate to severe calcium deposition in the fatty plaques.
There are 3.5 million interventional procedures done in heart arteries and 1.5 million in leg arteries annually. Out of a total of 5 million procedures; 1.7 million procedures may benefit from Shockwave Medical’s lithotripsy annually worldwide.
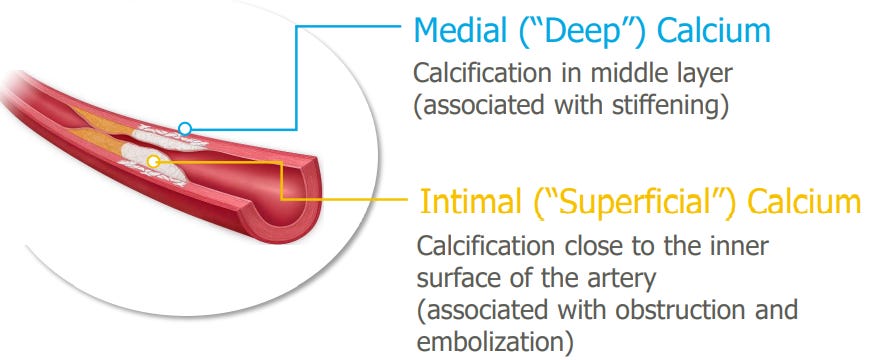
Pathophysiology of Plaque buildup in arteries:
At the initial phases of plaque development; only fat deposition takes place and later calcium starts depositing making it harder.
When physicians encounter these types of plaque, the presence of hard calcium becomes a barrier to implant the stent as the stent will not sufficiently expand in the presence of calcium as shown below:
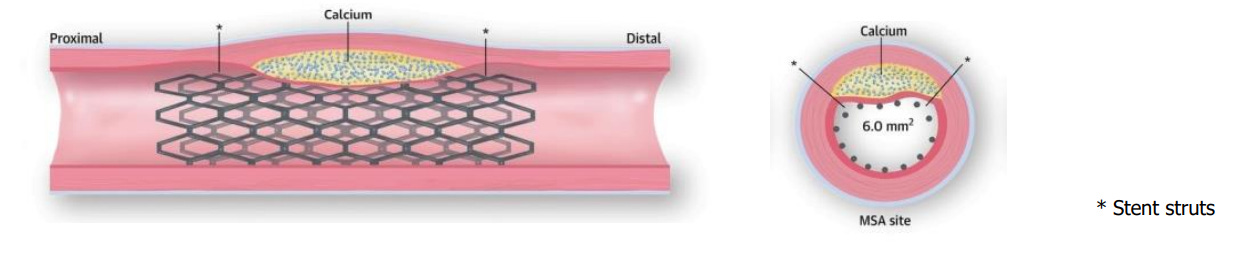
If you carefully look at the stent in the image on the right; you can notice a gap between vessel wall and the stent. The stent (asterix) does not fully cover the lumen which leads to poor outcome for the patients.
Traditional tools available are with serious risks as shown in the picture below:
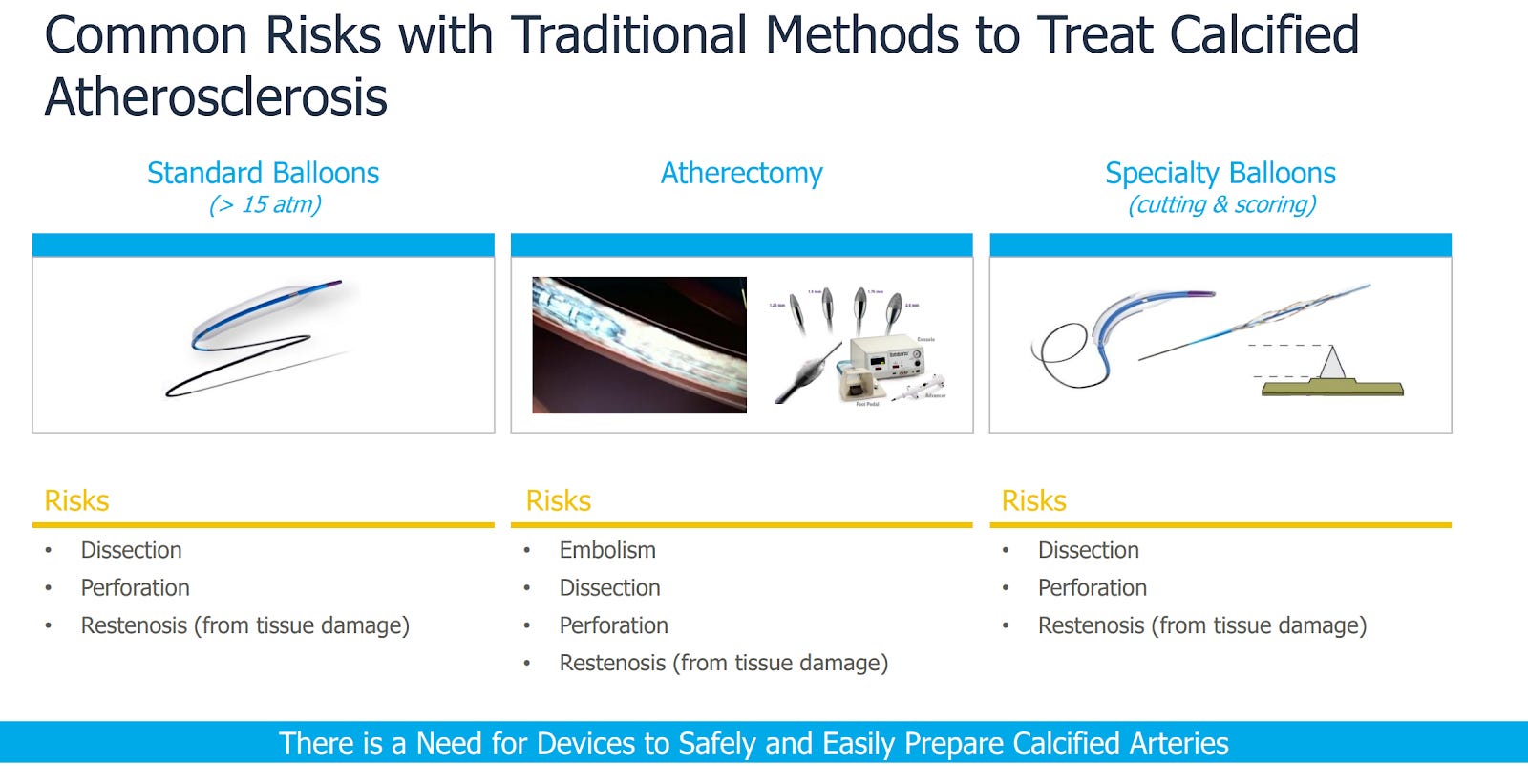
All of these tools listed above have complications like tearing the blood vessel and restenosis even after implanting the stent.
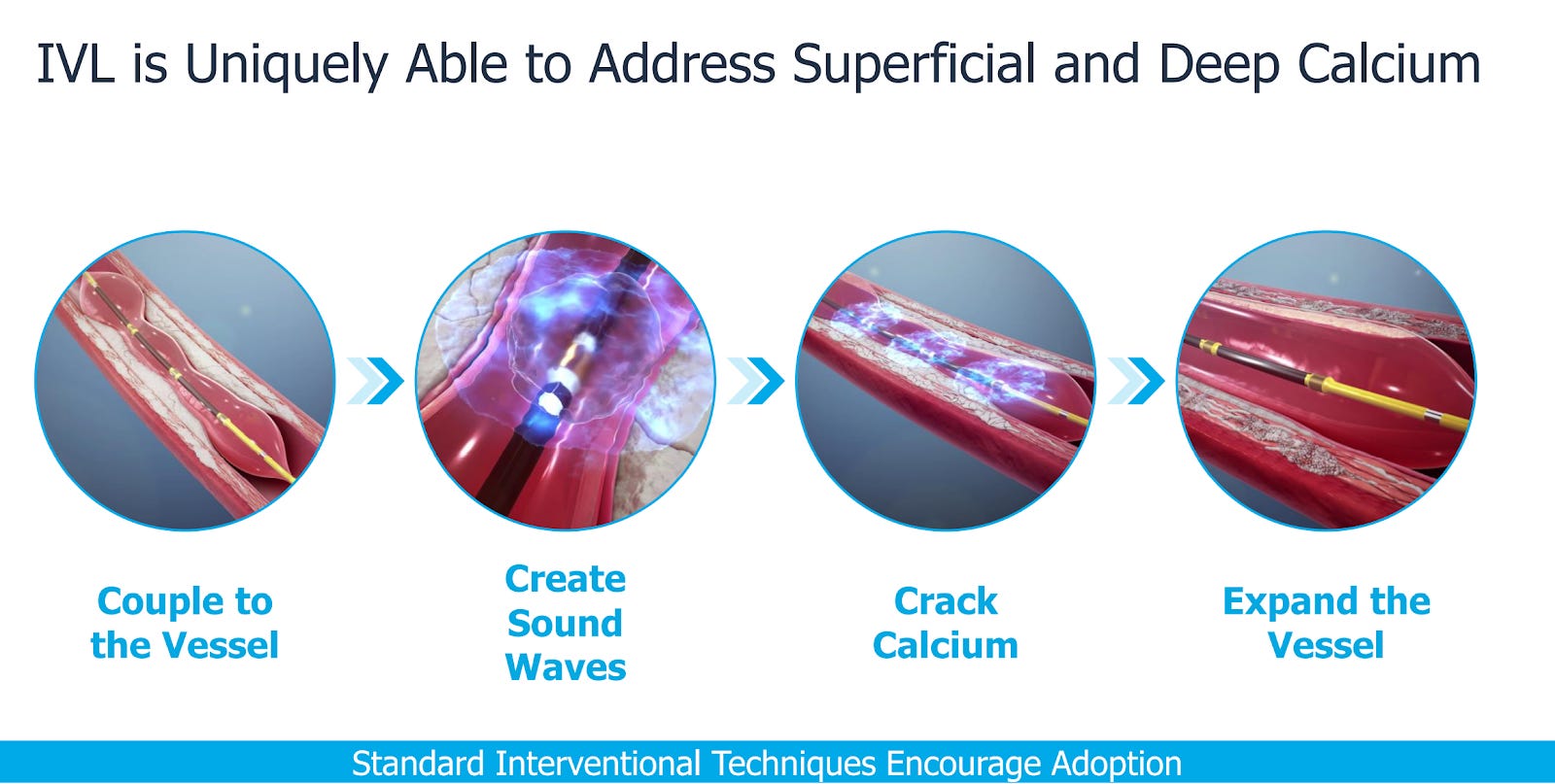
Lithotripsy on the other hand uses sound waves to crack the calcium without harming the tissue.
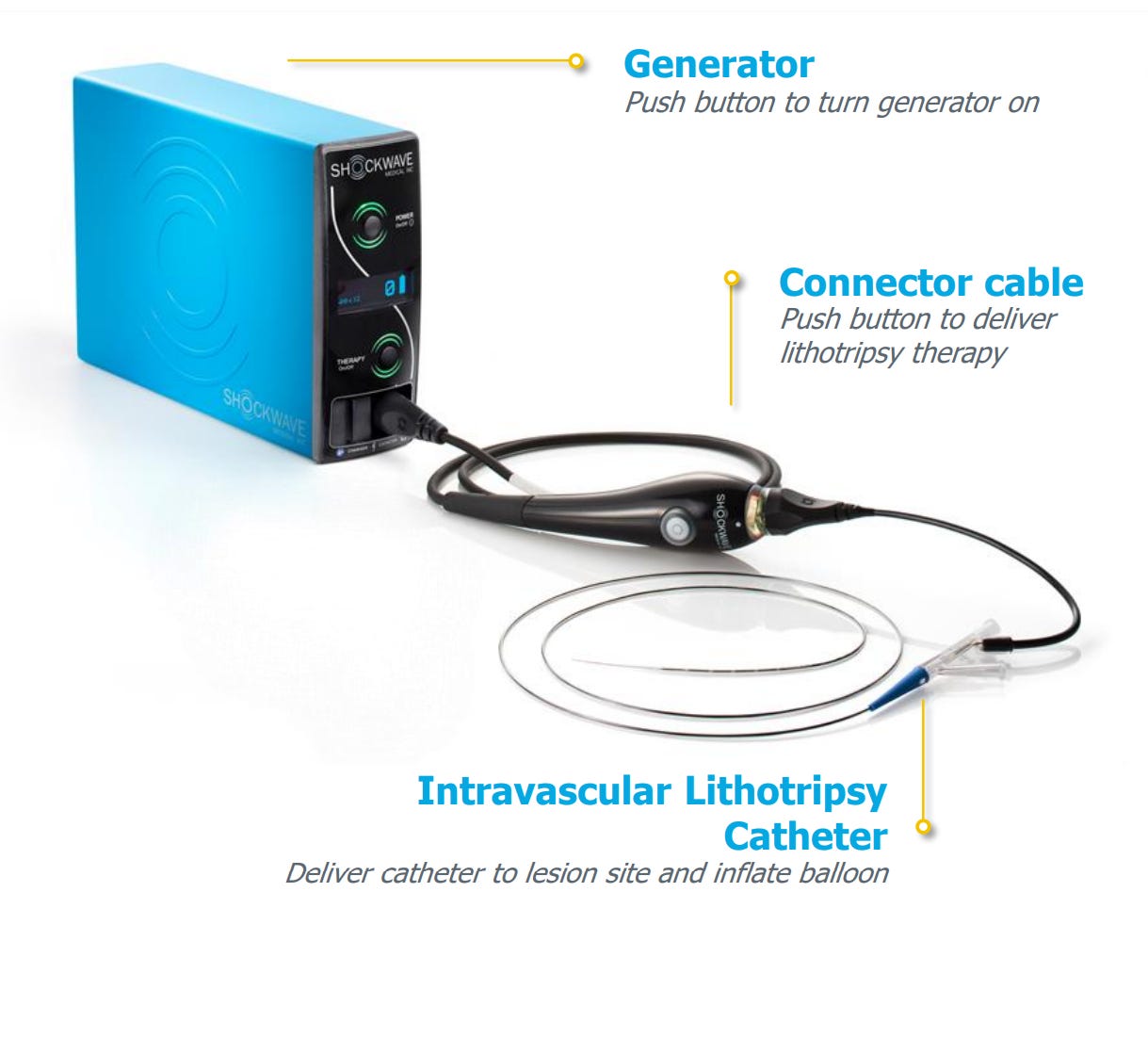
Intravascular shock wave lithotripsy uses only sound waves; it causes less damage to the blood vessel as well as expand the vessel so stent can be deployed properly.
Intravascular lithotripsy has been shown to be effective and safe therapy in treatment of severe calcium in blockages in both heart and leg arteries.
Expert analysis published in American College of Cardiology website acc.org (https://www.acc.org/latest-in-cardiology/articles/2020/07/17/08/00/intravascular-lithotripsy-in-cardiovascular-interventions) concluded that IVL is an intuitive and attractive modality for the treatment of severely calcified lesion that combines the calcium-disrupting capability of lithotripsy with familiarity of balloon catheters. This is a very encouraging endorsement by the experts in the field. Actually after reading this article in July 2020 I became bullish on the stock and started position right away. It has already become multi-bagger stock for me.
On Feb 16, 2021 FDA approved ShockWave medical’s catheter for calcium disruption in heart arteries. FDA had already approved their catheter for peripheral arteries disease treatment in 2016.
Financials and Valuations
Current market cap of SWAV is about 4 billion dollars and trades around EV/Sales LTM of 61! And EV/Sales of NTM of 35. This looks very expensive but if you look at the TAM of about 6 billion and remaining growth that is ahead; it may appear reasonable. Analysts are estimating 2022 revenue of 200 million. This translates to revenue multiple of about 20 which seems not cheap but reasonable. With total addressable market of 6 billion annually, at scale if company is able to capture 20% of the market, then their revenue could ramp up to 1.2 billion dollars. Suddenly this market cap of 4 billion may now appear reasonable. The stock has pulled back recently giving investors opportunity to accumulate shares at cheaper price than investors who bought few weeks ago.
I am long SWAV.
Disclaimer: The stocks mentioned in my newsletters are not intended to be a list of buy recommendations but rather some ideas for your watchlist. Perhaps they end up in your own portfolio after you conduct your own research and due diligence. Some of the stocks mentioned in my newsletters have smaller market capitalizations and therefore can be more volatile. I always encourage everyone to do their own research and due diligence before buying any stocks mentioned in my newsletters. Please manage your portfolio and position sizing in accordance with your own risk tolerance and investment objectives.
As a young anatomist and scientist, I see calcium plaques starting from ascending aorta to medium/small sized arteries of all sonar bodies beyond 65yrs old. As calcium scan becomes a norm, I believe more and more physicians will recommend removal of calcium plaques to avoid future life-threatening complications!